BLS pediatric algorithm
Last updated: March 15, 2022
Version control: Our ACLS, PALS & BLS courses follow 2020 American Heart Association Guidelines for CPR and ECC. American Heart Association guidelines are updated every five years. If you are reading this page after December 2025, please contact support@ACLS.net for an update. Version 2021.01.c
Pediatric basic life support for healthcare providers
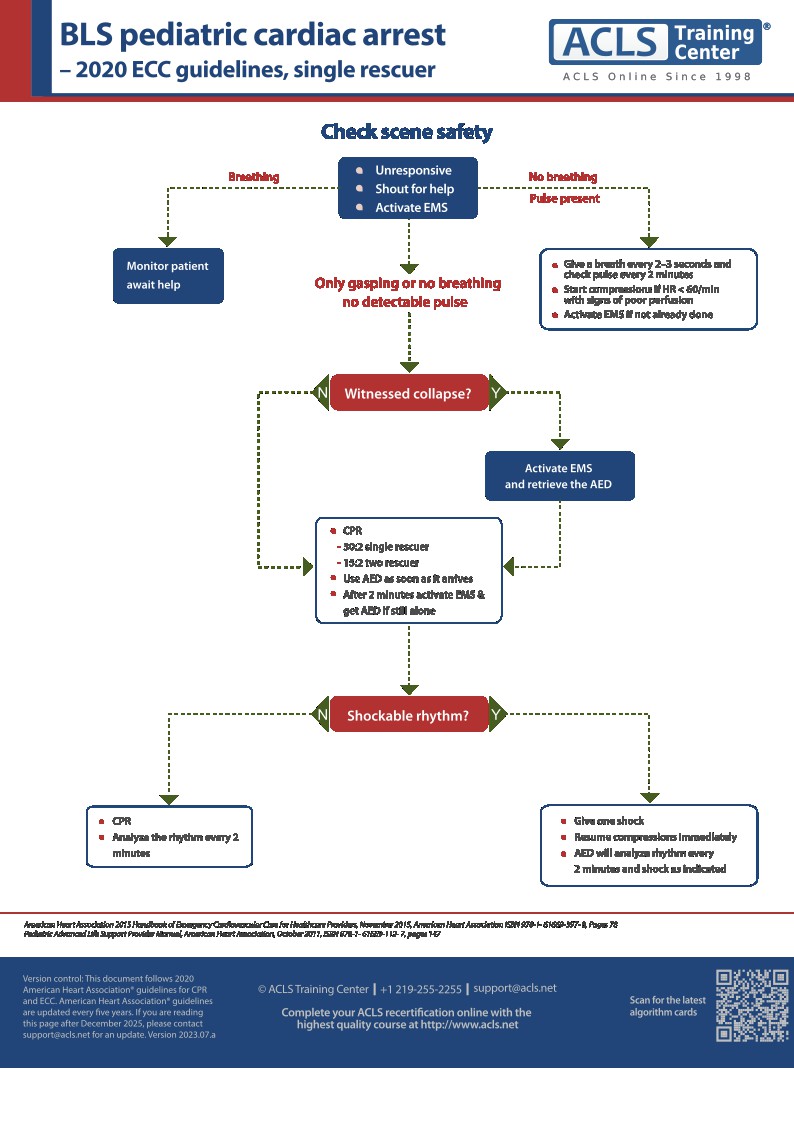
In Pediatric Basic Life Support for Healthcare Providers (HCP), the rescuer should first determine quickly if the victim is unresponsive. The provider should note if the victim is not breathing or is only gasping.
If the victim is not breathing, only gasping, or is unresponsive, with sudden collapse, a lone rescuer should activate the emergency medical response service and retrieve the automated external defibrillator or defibrillator. If there is another rescuer, that person should activate EMS and retrieve the AED or defibrillator. If the victim did not experience “sudden” collapse, the rescuer should perform CPR for 2 minutes prior to seeking a defibrillator.
Emergency care providers should check the victim’s pulse for at least 5 seconds but no longer than 10 seconds. For children aged one to adolescence, the pulse should be checked at the carotid artery. In infants, the brachial pulse should be assessed.
If there is a palpable pulse within 10 seconds, then a rescue breath should be given every 2-3 seconds. Breaths should last one second and the chest should be observed for visible rise.If the victim has an advanced airway, then the provider should administer a breath every 2-3 seconds.
If the pulse is less than 60/minute, or if the victim has signs of poor perfusion after adequate ventilation and oxygenation, the provider should begin chest compressions. In the absence of a pulse, a lone rescuer should begin CPR with 30 high quality compressions followed by two breaths. If two healthcare providers are available, the cycle of compressions to breaths should be 15:2 (pediatrics).
High quality compressions in CPR should be a minimum of 1/3 the AP diameter of the chest, or approximately 1 ½ inches in infants (4 cm) and 2” in children from age one to adolescence. The rate of compressions should be 100–120 per minute. Chest recoil should be complete between compressions.
Pediatric compression is performed with the head of one hand over the lower ½ of the sternum, between the nipples. In infants, use two fingers, or use the thumb encircling technique if multiple providers are available.
After two minutes have passed, if EMS has not been notified, then they should be called. At this time, if the AED is not yet available, the rescuer should retrieve it. When the AED is available, the victim’s rhythm should be quickly assessed.
Shockable rhythms include ventricular fibrillation or pulseless ventricular tachycardia. One shock should be given to the victim, with resumption of CPR immediately after the shock. CPR should continue for 2 minutes. A dose attenuator should be used on infants if available, but if not, adult pads can be used.
If the rhythm is not shockable, CPR should be resumed immediately. The heath care provider should check the rhythm once more after two minutes of CPR (5 cycles of 30:2). This should until the victim moves or until advanced life support is available.
The airway in pediatrics should be opened with a head tilt/chin lift for children over the age of one, and with the infant in the sniffing position. If trauma is suspected, then a jaw thrust should be used to open the airway.
For more information on getting certified, check our BLS and CPR courses. Our courses are 100% online and accepted in all US states and Canadian provinces.
PDF version
Order the full set of printed crash cart cards

Planning to certify/recertify ACLS?
Get a reminder when you need to take the exam

Written by Jessica Munoz DPN, RN, CEN, providing nurse training at Yale New Haven Health-Bridgeport Hospital since 2022. Previously in healthcare and education at Griffin Hospital, St. Vincent's College of Nursing and Sacred Heart University Medical Center.
More by this author: